Cette page a été traduite automatiquement.
Merci de bien vouloir compléter un sondage de 1 minute concernant la qualité de cette traduction.
Simulation de chirurgie en 3D pour la conception de nouveaux dispositifs médicaux
Validation virtuelle de la chirurgie robotique en cabinet

Tout comme les callosités qui se forment sur la main, la surutilisation de la voix peut entraîner des excroissances dures et non cancéreuses sur les cordes vocales. L'élimination rapide de ces nodules afin de préserver la fonction des cordes vocales est essentielle pour les acteurs et les chanteurs qui dépendent de leur voix. La méthode traditionnelle pour retirer les nodules bénins, ainsi que certaines tumeurs cancéreuses rares, est la chirurgie au bloc opératoire d’un hôpital.
Ces dernières années, l'élimination au laser de ces lésions dans les cabinets médicaux a gagné en popularité. La procédure consiste à détruire les excroissances des cordes vocales avec des impulsions laser pour les éliminer ou les rétrécir. Il peut s’agir d’une intervention chirurgicale ambulatoire rapide qui ne nécessite pas d’anesthésie générale.
Cependant, la technologie des dispositifs endoscopiques utilisée pour les procédures actuelles présente des limites. « Cela fonctionne. C'est une bonne nouvelle », déclare Loris Fichera, professeur d'ingénierie robotique au Worcester Polytechnic Institute (WPI). « La mauvaise nouvelle est qu'il peut être difficile d'atteindre certaines parties du larynx car les instruments sont très limités dans la manière dont ils dirigent la lumière. »
Les nouvelles conceptions de fibres optiques et configurations d’endoscopes devraient surmonter cette limitation. Fichera et ses collègues ont utilisé MATLAB® pour simuler la manière dont les fibres à pointes inclinées, au lieu des fibres plates utilisées aujourd'hui, fonctionnent dans les modèles 3D haute définition des cordes vocales humaines, ou du larynx. En simulant les dispositifs médicaux, ils espèrent réduire le temps et les coûts nécessaires à la fabrication de prototypes physiques qui doivent être testés d'abord sur des corps de donneurs, puis en clinique. Les simulations pourraient fournir une validation lors du développement futur de fibres optiques et d’instruments endoscopiques plus efficaces.
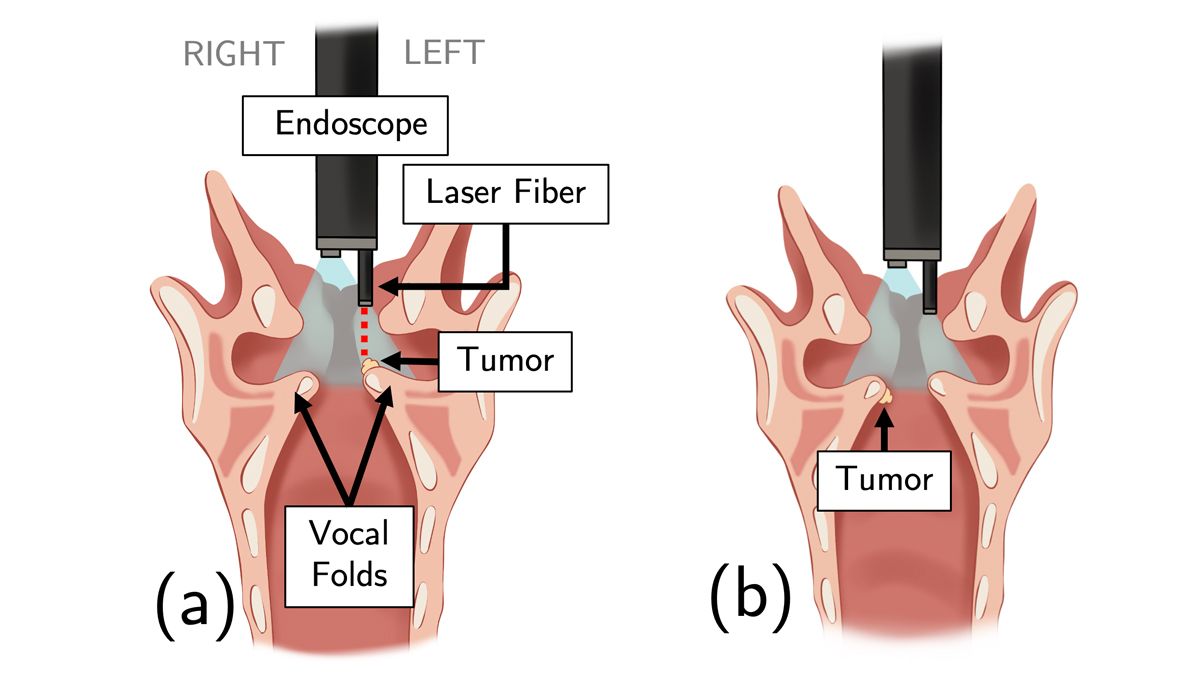
a) Le cône bleu représente la vue de la caméra endoscopique, qui inclut une vue de la tumeur. La ligne pointillée rouge représente la ligne de visée de la fibre laser. b) Une tumeur située sous la corde vocale est moins accessible à la fibre laser orientée vers l'avant. (Crédit : Illustration de Carla Dipasquale, avec l'autorisation de Loris Fichera)
« Ces dispositifs sont très onéreux et nécessitent beaucoup de temps à fabriquer », explique Fichera. « Grâce à la simulation avec MATLAB, nous pouvons évaluer rapidement des dizaines de conceptions différentes sans les fabriquer. Nous déterminons quelle configuration est prometteuse et celle que nous devrions prototyper. Cela réduit le temps de prototypage, ce qui le rend beaucoup plus rentable. Chaque cycle de conception et de prototypage ne prend désormais que trois semaines à deux mois, selon la complexité de la conception. »
Larynx virtuelle
La chirurgie clinique du larynx consiste à introduire dans la gorge un endoscope fin et flexible portant une caméra et une fibre optique. Les fibres optiques actuelles ont une extrémité plate et émettent de la lumière vers le tissu cible, de sorte qu'elles ne peuvent pas atteindre la surface inférieure ou les bords des cordes vocales qui ne sont pas en ligne de mire directe.
« Avec Medical Imaging Toolbox, nous pouvons charger l'ensemble des données et créer le rendu tridimensionnel en quelques clics seulement. Posséder cette fonctionnalité et la possibilité d'exporter des données est important : cela signifie que nous ne partons pas de zéro pour chaque nouveau design. Nous pouvons compter sur quelque chose dont nous savons qu’il fonctionne et qui est standard. Cela permet de gagner des semaines pour chaque nouvelle conception. »
Des recherches récentes ont suggéré que les pointes effilées des fibres qui dirigent la lumière sous différents angles pourraient permettre aux médecins de traiter les espaces difficiles d'accès du larynx. Fichera s'est associé à des professionnels de la santé de la Harvard Medical School et du Brigham and Women's Hospital de Boston pour évaluer l'efficacité de ces fibres inclinées. Ils ont mené une étude basée sur la simulation comparant différents types de fibres laser : une fibre traditionnelle orientée vers l'avant et trois fibres à tir latéral qui émettent de la lumière à des angles de 45°, 70° et 90°, respectivement.
L'équipe WPI a créé sept modèles anatomiques 3D différents du larynx humain en compilant des images de tomodensitométrie (microCT) d'échantillons de larynx et en les traitant avec Image Processing Toolbox™.
La tomodensitomètrie est une séquence d'images 2D en niveaux de gris haute résolution dans laquelle chaque pixel transmet la densité du tissu à un endroit donné. Chaque image représente une tranche de tissu distante de quelques micromètres de la tranche de l'image suivante. « C'est comme si des photos étaient prises à différentes hauteurs », explique Fichera. « Nous traitons ces images pour reconstruire la forme tridimensionnelle, et le résultat est un fichier stéréolithographie, ou STL, le même format que celui normalement utilisé pour l'impression 3D. »
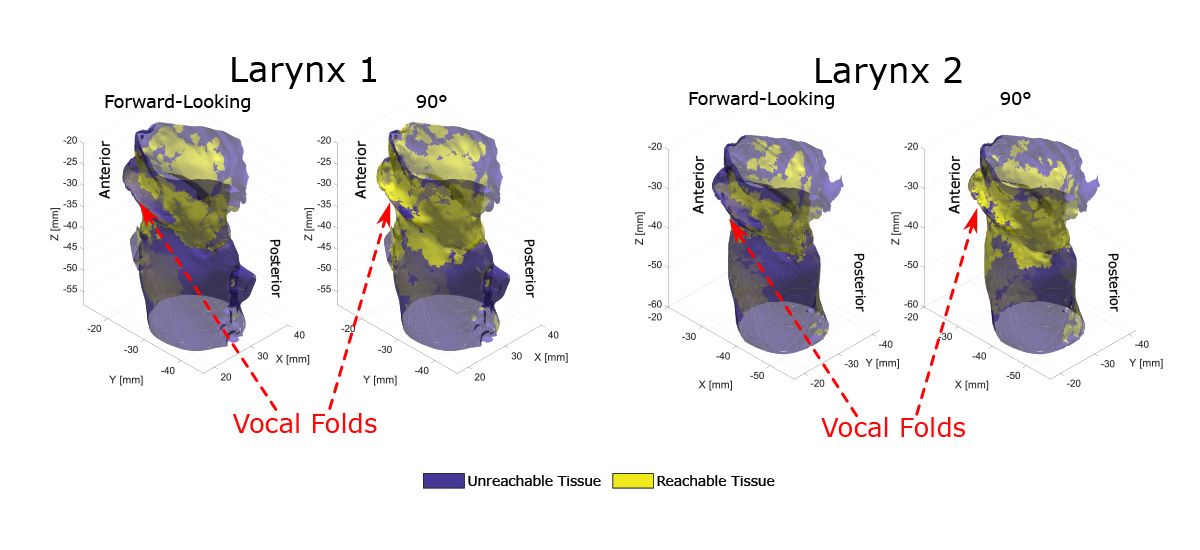
La fibre à tir latéral à 90° peut accéder à des zones du larynx auparavant inaccessibles. (Crédit : Loris Fichera)
Les logiciels de radiologie commerciaux peuvent reconstruire des formes 3D à partir d’images médicales. Néanmoins, le logiciel est difficile à utiliser et ne peut souvent pas exporter les données au format STL requis par Fichera et ses collègues. L’équipe a passé une semaine à écrire du code pour convertir les tomodensitométries en rendu 3D du larynx.
« Avec Medical Imaging Toolbox, nous pouvons charger l'ensemble des données et créer le rendu tridimensionnel en quelques clics seulement. Posséder cette fonctionnalité et la possibilité d'exporter des données est important : Cela signifie que nous ne partons pas de zéro pour chaque nouveau design. Nous pouvons compter sur quelque chose dont nous savons qu’il fonctionne et qui est standard. Cela permet de gagner des semaines pour chaque nouvelle conception », explique Fichera.
Les étudiants diplômés de Fichera utilisent également Medical Imaging Toolbox™ pour le cours sur les robots chirurgicaux. Dans le passé, les étudiants devaient pratiquer la reconstruction tridimensionnelle à l’aide d’un logiciel de radiologie. « Ils n'ont plus besoin d'utiliser ce logiciel », déclare Fichera. « Je leur demande d'utiliser MATLAB pour cela. »
Simulation de chirurgie
Après avoir créé les modèles de larynx virtuel, l'équipe WPI a utilisé le code open source MATLAB de File Exchange pour créer un modèle d'endoscope commercial couramment utilisé. L'endoscope a la pointe de la caméra sur la corde vocale droite et la pointe de la fibre laser sur la gauche. Il se déplace avec trois degrés de liberté.
« Avec Parallel Computing Toolbox, la simulation prend environ sept heures. Sans calcul parallèle, cela prendrait beaucoup plus de temps, probablement plusieurs jours. »
L'équipe a créé un programme pour simuler l'insertion et le mouvement de l'endoscope dans le larynx à l'aide d'un algorithme de planification de mouvement. Les chercheurs ont déployé les endoscopes virtuels avec les différentes fibres optiques dans les sept modèles de larynx. Le programme a produit un nuage de points représentant tous les endroits du larynx que les instruments peuvent atteindre.
Ensuite, ils ont utilisé la projection de rayons – une technique informatique largement utilisée par les développeurs de jeux pour simuler l’éclairage dans une scène virtuelle 3D – pour imiter le faisceau laser émergeant de l’extrémité de la fibre optique. Ils ont utilisé un algorithme d’intersection rayon-triangle pour détecter le tissu du larynx atteint par le faisceau laser. « Essentiellement, nous parcourons chacun de ces points nuageux un par un et demandons : « OK, si notre fibre laser est ici et que nous appliquons de la lumière à partir de cet endroit, quel tissu pouvons-nous atteindre ? » »
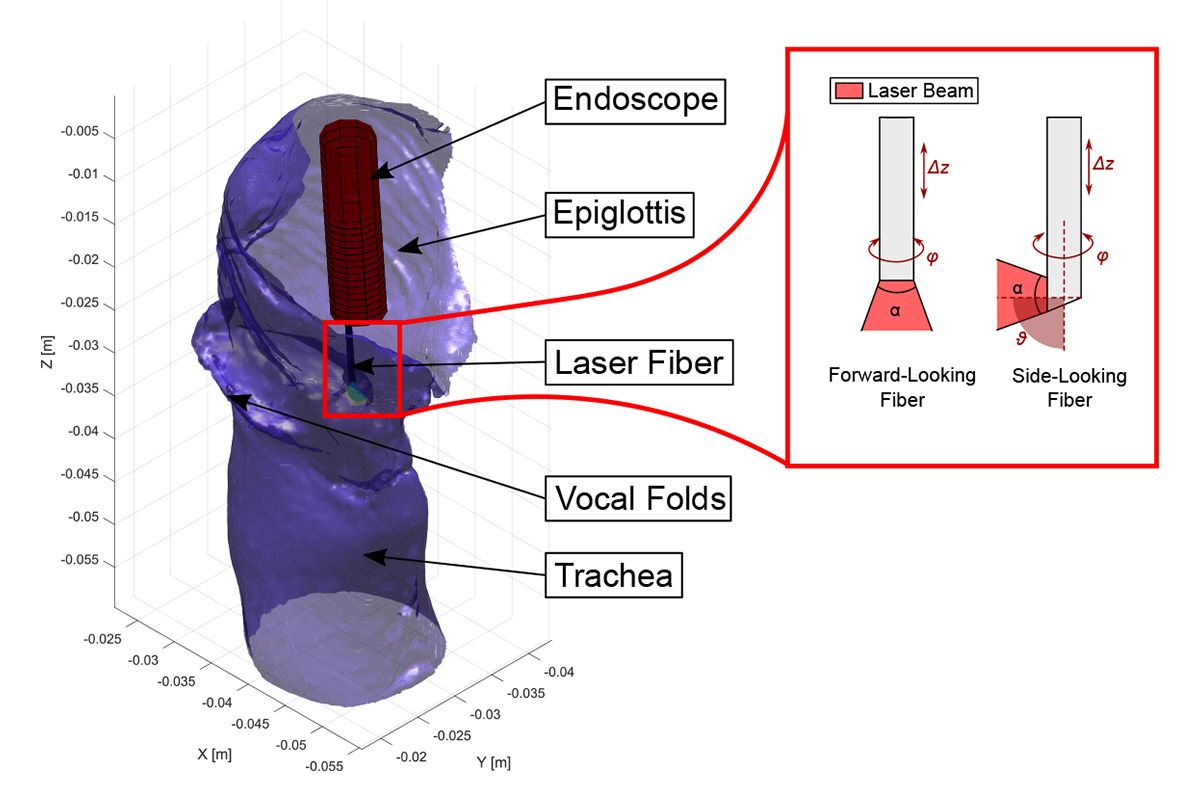
Le modèle d'endoscope montrant les degrés de liberté de la fibre. (Crédit : Loris Fichera)
La projection de rayons est coûteuse en termes de calculs, dit-il, c'est pourquoi ils ont utilisé Parallel Computing Toolbox™ pour accélérer les choses. « Au lieu de parcourir des milliers de points de vue et de projeter des rayons lumineux un par un, nous diffusons des rayons en parallèle depuis autant de points que possible à la fois, puis nous regroupons tous les résultats. Avec Parallel Computing Toolbox, la simulation prend environ sept heures. Sans calcul parallèle, cela prendrait beaucoup plus de temps, probablement plusieurs jours. »
Ils ont constaté que les fibres coudées à 45°, 70° et 90° augmentaient la quantité totale de tissu laryngé accessible et traité en moyenne de 50 %, 74 % et 84 %, respectivement.
Concevoir des endoscopes de nouvelle génération
En plus de fournir la preuve que les fibres à tir latéral pourraient améliorer la chirurgie robotique du larynx, l'étude a révélé une limitation fondamentale des endoscopes actuels. Les simulations chirurgicales ont montré un écart flagrant dans le nuage de points près de la corde vocale droite. « Le logiciel nous disait qu'il y avait une partie du larynx très difficile à atteindre », explique Fichera. « Donc, si un patient présente une tumeur ici, vous ne pouvez pas la traiter. Cela n’avait aucun sens et la première chose que nous avons pensé, c’est que nous avions dû faire une erreur. »
« Notre idée est de remplacer l'endoscope utilisé aujourd'hui par notre propre version de cet appareil. Quelle que soit la conception que nous proposons, nous pouvons d'abord effectuer une simulation dans MATLAB avant de fabriquer ou même de toucher un instrument physique, voir s'il fait ce que nous pensons, puis passer au prototypage. »
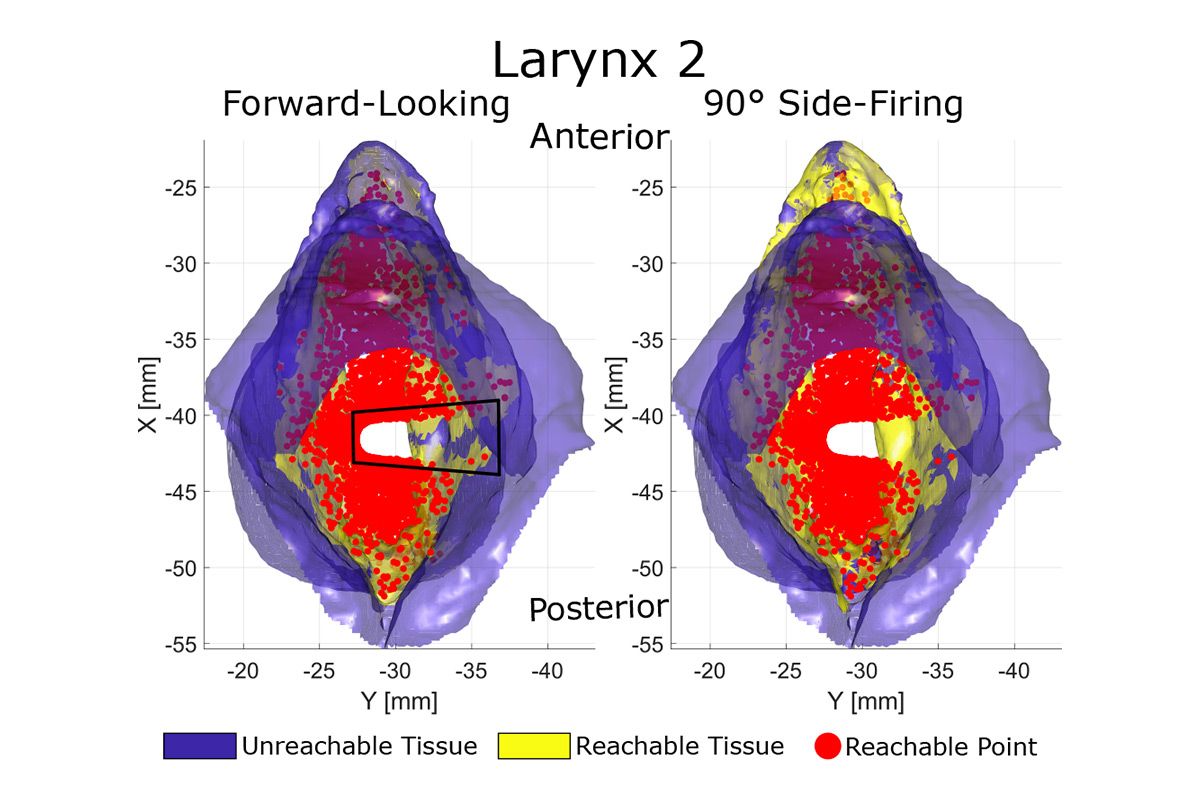
Les simulations chirurgicales ont identifié une lacune dans le nuage de points près de la corde vocale droite à laquelle les endoscopes actuellement disponibles ne peuvent pas accéder. (Crédit : Loris Fichera)
À leur grande surprise, les collègues médecins de Fichera ont confirmé qu'ils ressentaient effectivement ce manque d'accès à la corde vocale droite. En revenant au programme informatique, l'équipe de Fichera a réalisé que cet écart était dû à la conception excentrique de l'endoscope, avec la caméra d'un côté et la fibre optique de l'autre, et au fait qu'il est difficile pour les chirurgiens de faire pivoter complètement l'endoscope de 360°.
Fichera affirme que les endoscopes utilisés aujourd'hui pour la chirurgie laryngée sont basés sur la conception d'autres endoscopes au lieu d'être optimisés pour cette procédure spécifique. L’équipe WPI prévoit d’utiliser son étude comme base pour développer de nouveaux dispositifs médicaux endoscopiques.
« Nous avons commencé cette recherche en pensant que tout ce que nous avions à faire était de développer une nouvelle fibre tout en continuant à utiliser les mêmes instruments », explique-t-il. « Mais en fin de compte, je pense que ces résultats nous disent également que nous devons également repenser la conception de l'endoscope. »
Fichera et ses collègues prévoient d'utiliser leurs données pour demander des subventions et utiliser le financement pour développer un tout nouveau dispositif. « Notre idée est de remplacer l'endoscope utilisé aujourd'hui par notre version de cet appareil. Quelle que soit la conception que nous proposons, nous pouvons d'abord effectuer une simulation dans MATLAB avant de fabriquer ou même de toucher un instrument physique, voir s'il fait ce que nous pensons, puis passer au prototypage. »

Lire d'autres articles
ÉQUIPEMENTS MÉDICAUX
Le Machine Learning aide un neurochirurgien lors d'une chirurgie du cerveau
Améliorer la chirurgie de la maladie de Parkinson grâce à l'IA et au traitement du signal
ÉQUIPEMENTS MÉDICAUX
Le Machine Learning aide à réparer les cœurs malades
Une start-up fait entrer le traitement de l'arythmie dans le 21e siècle